
First and foremost, complaint handling is a business and regulatory requirement. If you are going to be in the medical device business, you must document a process for gathering feedback. If you are new to complaint handling, you will first want to start by reading the requirements for complaint handling as spelled out in US FDA regulation 21 CFR Part 820.198 and Clause 8.2.2 of ISO 13485:2016. (The ISO 13485 standard is a copyrighted document so you won’t find the text online, but you can buy it from ISO.)
The word “gather” is important because it implies we are proactively seeking feedback. Complaints, unfortunately, come to us, so complaint handling is a reactive procedure. Let’s take a quick look at the definition of complaint handling according to ISO 13485:2016 and 21 CFR Part 820.
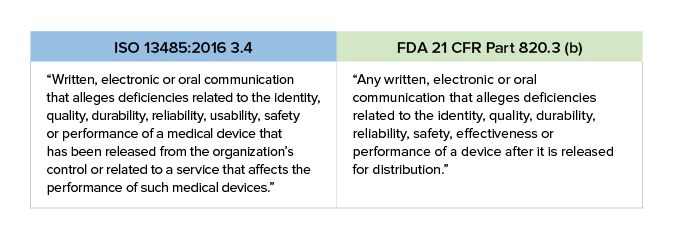
One thing you should note is the inclusion of the word “usability” in ISO 13485:2016. This is an increasingly important issue to which you need to pay attention. The US FDA refers to usability as “Human Factors.”
Essentially, postmarket issues can be placed into one of two buckets. The first type is an “incident-driven” issue. For instance, let’s say you receive a report from a hospital that an electrical malfunction has occurred in your surgical ablation system tool. The failure could have led to serious harm or death for the patient. This is an incident-driven issue that requires immediate action.

The second type of issue that arises is one driven by a review of data. For example, while reviewing service records you may notice a trend in repeated failures of your surgical ablation pens under certain conditions, which qualifies as a complaint. That’s certainly a reliability problem and falls within the ISO 13485:2016 and FDA definitions of complaints.
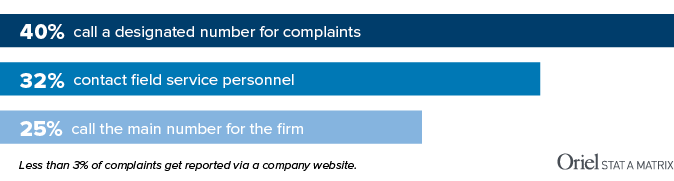
You may assume that the majority of complaints get reported via the “contact us” form on a company website or a specific email address posted online. Believe it or not, only 3% of medical device complaints come via these channels. In the medical device world, the telephone still reigns supreme. Nearly two-thirds of complaints are reported by telephone. Surprised? The reality is that when people experience a problem with a device, they want to talk to a real person about it right now, not submit an anonymous online form/email into a black hole.
In our increasingly impersonal online world, the process of fielding phone calls from angry customers may seem time-consuming and unpleasant, but it’s worth it. You WANT people to call you because it gives your team an opportunity to ask questions and dig into the underlying issue. A good service rep – trained to listen, probe, and show empathy – can dilute the venom of an upset customer while gathering the data needed to further investigate the claim.
Before we talk about reporting, we should take a look at the basic complaint-handling process, which has three phases.

STEP 1 Intake – This is where you do initial triage. Is the complaint valid? Is it potentially reportable? Was it caused by use error or abnormal use?
STEP 2 Investigate -This is where you dig in. How deep you go will depend on the nature of the complaint. In many cases, you will conduct an initial investigation and determine that no further research is necessary. On the other end of the spectrum are incidents where harm was done to a patient or user. These need to be thoroughly investigated to determine the root cause of the issue.
STEP 3 Close – After you determine the level to which you need to investigate and have assembled the appropriate documentation as required, you will “close” the complaint. While you are investigating and closing complaints, you may also be updating your risk management files, preparing a vigilance report, and/or – in extreme circumstances – taking immediate action to mitigate further harm.

You may be able to close the complaint after an initial investigation into assignable cause. Is there an open CAPA for this issue? Does the complaint suggest that a closed CAPA action was ineffective? Is this being investigated by another entity, such as a supplier or distributor? Make sure you understand when to escalate to Level II and when an initial investigation is enough. In all cases, document, document, document.
After your initial Level I investigation, you may find it necessary to investigate the probable cause to find out if there is a new problem. That’s usually due to the fact that a new (previously unreported) issue has occurred, or your trend alerts have been exceeded. At this point you may choose to end an investigation because the failure is within the limits you have established based on labeling, intended use, and risk files. Or, you may have a situation in which the failure is a known issue but falls outside a risk threshold or trending (frequency) limits. These risk thresholds or trending limits are outputs of your risk management process. For example, in design you reduced the risk of battery failure by adding a backup battery, but you still want to trend failures of the first battery. The failure rate is pretty low, as expected, but then you see a sudden shift upward in the occurrence rate. This triggers you to investigate, uncovering a supplier issue and allowing you to solve the problem before any patients are harmed.
If your Level II investigation reveals that you have a new failure mode on your hands, you may need to take the next step and open a CAPA. You certainly need to update your risk management file. Before doing so, you need to define the problem and then investigate its root cause. You will also need to determine whether a recall is needed or if some other corrective/containment action is warranted. It’s important to know that not all complaints require a root cause investigation or CAPA! That being said, there are some events that may require a root cause investigation:

US OfficeWashington DC
EU OfficeCork, Ireland


